
Tongue to Toes: How Does This Matter?
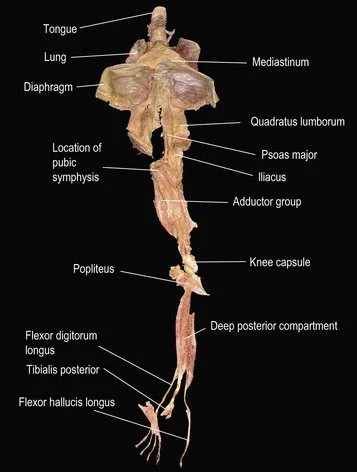
Over the past few years, this graphic has appeared in various groups and is often used to support the promoted group model. The fascial communities posted this graphic to validate the need for whole body fascial work to release the entire person, not just where the problem is noted, despite a lack of quality evidence showing that we can permanently change the length of connective tissue, as taught in most fascial lines of training. (Do you have studies that prove this? Drop them in the comments. Their "find the pain/reported problem, look elsewhere for the cause" is a weak attempt to justify their views. Actual causation is complex and is never a simple story of a fascial restriction (1).
More recently, this graphic has been circulating in groups and posts about tongue-related models of care, including those working with tongue-tie release patients. The presence of "connection" from tongue to toe seems impressive, though possibly less so if we ask the people posting this meme how it matters. Those validations should be attached to the meme if this connection is a proven, solid reason for a condition or problem, and supports our intervention beyond group speak. The entire body is connected, which certainly matters, but how is this one specific connection relevant? Tongue tie laser/surgical releases may be one of the few instances where this vague concept may matter. However, how does this graphic guide your practice short of a surgical release? What evidence (not perspectives) exists to justify reposting this meme? Without this background evidence, this meme is meaningless.
Addressing the "whole body" is another claim many groups make. Do these claims move beyond theoretical or consensus-building? Or are they simply justification models used to support their beliefs, claims, and actions? Human beings benefit from numerous yet disparate models of care, including exercise, manual therapy, and education. My myofascial release training taught me to look broadly, as balancing an asymmetrical pelvis was said to be key to resolving headaches and other issues. Those perspectives, when actioned, often did help headaches, but so do other intervention models that pay no attention to balancing the pelvis. The discrepancies between a model's claims and the overall outcome, as observed through various perspectives and therapy models, should be concerning. They concern whether one removes the blinders imposed by their chosen intervention tribe. Treatments for the tongue of various types are highly effective for pain, poor motor control, limited articulation, swallowing disorders, voice fatigue-related concerns, sensory awareness, changes in resting posture, and more. But is that tongue-to-toes correlation just that, a correlation? Or is there substantial causative data to lead us to support this broadly interpretable image?
Walt Fritz, PT
1. Anjum, R. L., Copeland, S., & Rocca, E. (2020). Rethinking causality, complexity and evidence for the unique patient: a Causehealth resource for healthcare professionals and the clinical encounter (p. 241). Springer Nature.